
Part 1 | The Dirty Words in Healthcare: Unpacking Utilization Management & Prior Auth


The Evolution of UM – From Cost Containment to Value Creation
Utilization Management (UM) was meant to promote high-value care and be the anchoring counter-balance to fight fraud, waste and abuse…but it has metastasized into a bloated cost center of its own. The U.S. spends over $93.3 billion annually across payers and providers implementing, contesting, and navigating utilization management. [1,2] Amidst this, 75% of prior authorization (PA) appeals are overturned and 1 in 3 physicians report witnessing serious adverse events due to authorization delays as highlighted by the American Medical Association. [3-5]
Additionally, the United States has spent two decades digitizing healthcare, only to discover that integration and automation without alignment doesn’t solve for friction, it just uncovers other issues or worse moves it faster and elsewhere.
This series reframes UM as a SYSTEM LOGIC PROBLEM, not just a process or technical flaw. Through this series we’ll explore its evolution, drive deeper foundational understanding, and map what needs to change if UM is to deliver on its original intent.
The Infrastructure Still Doesn’t Work
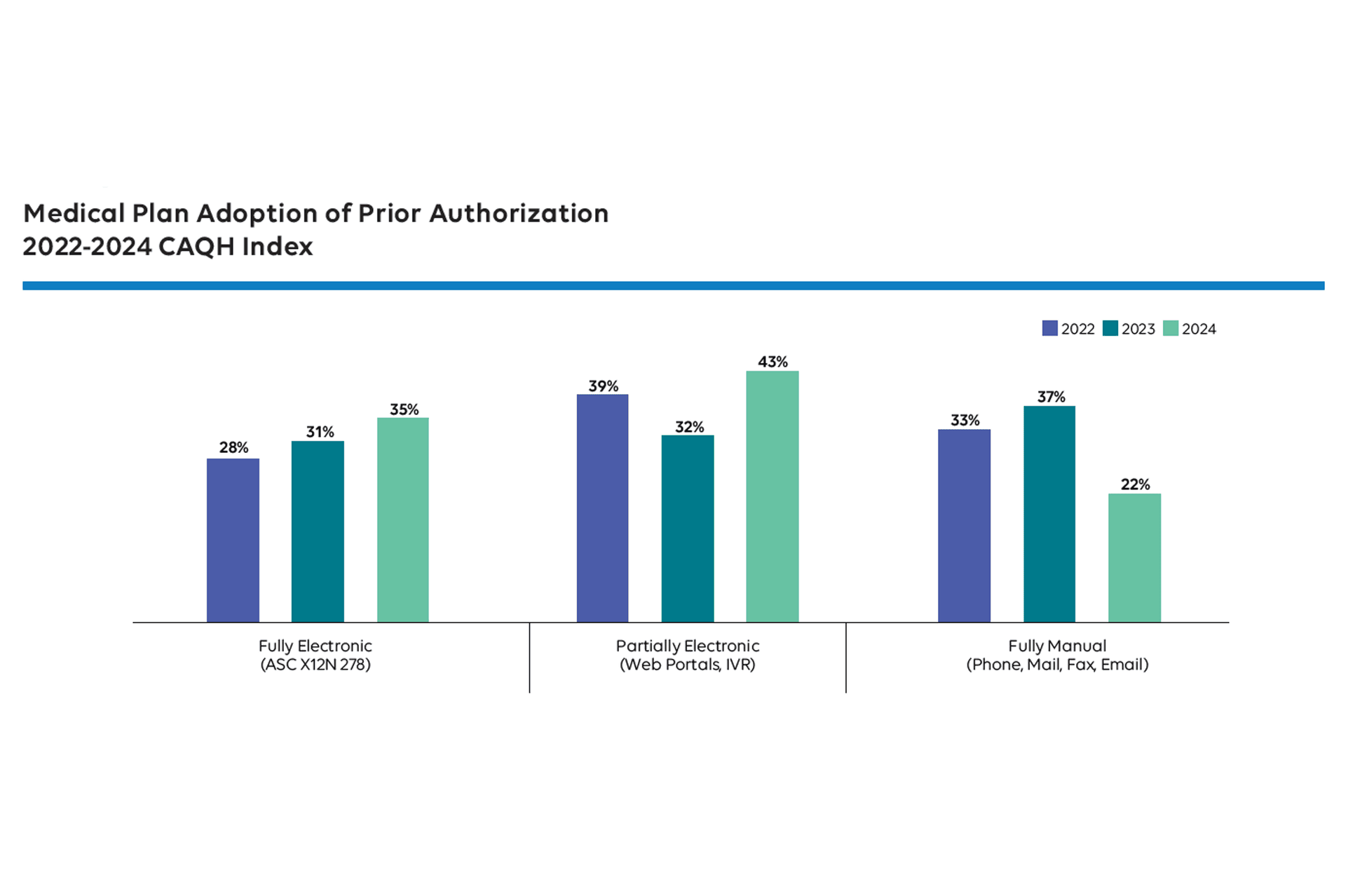
Despite massive investments in EHRs and payer portals, PA remains largely manual. According to the 2024 CAQH Index Report, only 35% of PA transactions were fully electronic, and manual transactions cost $10.92 vs $3.61 when done electronically. That makes PA one of the most expensive manual transactions in healthcare (see Figure 1).[6]
Even worse, clinical staff or provider access teams may spend an average of 12 hours per week managing PA, which is up from 10 hours in 2018.[3,7] Portals multiply instead of unify, faxes (or e-faxes) persist and peer-to-peer calls drag on sometimes evolving from RN-to-RN, or pharmacist-to-pharmacist, to MD-to-MD. Denial rationales are vague or missing and workflows varying by payer, geography, employer, and benefit and with variability into payer policy transparency and to make matters often worse, the patient and paying member often has to go through significant hurdles to gain access to the specifics of diagnostics or therapy medical necessity policies that govern their coverage.
Friction has not been eliminated, but rather we have just digitized it.
When Misalignment Becomes Harm
The consequences are not abstract. Denials and delays lead to worse outcomes, especially when at first patients are stable, the treatment plan is guideline-concordant, but time to therapy is critical.
- Prescription denials for certain medication classes including β₂-agonists, antiepileptics, and atypical antipsychotics were associated with 40-75% increased odds of acute care visits within 60 days [3]
- 60% of neurology studies on PA reported care delays, and 25% reported increased disease activity, including breakthrough seizures and multiple sclerosis relapses [4]
- In cancer care, 69% of patients perceive delays from PA, leading to increased anxiety and reduced trust [8]
- Systematic reviews across oncology, cardiology, pediatrics, and behavioral health show clear associations between PA and preventable hospitalizations, delayed therapy, and worse disease control [2,3]
These harms may not be intentional, but they are embedded in the reality of how UM has evolved. UM was originally introduced to reduce unnecessary utilization and rein in skyrocketing healthcare costs. As care delivery evolved and evidence-based medicine matured, UM promised to ensure that interventions were medically necessary, evidence-based, and aligned with the benefit design of each plan.
On paper, this sounds good, however instead of aligning incentives and workflows, it has added fragmentation. Over time, the focus shifted from clinical optimization to cost containment. UM is now the gatekeeper, not the guide. The administrative burden grows, and PA became its most visible symptom in UM.
Foundations First: Payers and Member Benefits
Every UM decision, whether it's about necessity, setting, or duration, passes through a complex operational filter rooted in the patient's specific benefits policy and design. That means the right clinical decision can still trigger a denial if it doesn’t align with the underlying patient’s/member’s policy architecture governing his or her coverage.
At its core, this is operationalized through a patient-specific overlay, which includes:
- Line of Business (LOB): Medicare Advantage, Medicaid (FFS or MCO), Commercial/ASO, Exchange plans each carry distinct policy constraints and turnaround requirements.
- Network Structure: Whether the plan is HMO, PPO, EPO, or POS determines the referral process, out-of-network allowances, and prior auth necessity.
- Benefit Design: This includes covered services, exclusions, tiered cost-sharing, utilization thresholds, and medical vs. pharmacy policy rules.
- Payer-Specific Rules: CMS timelines (e.g., MA’s 72-hour urgent PA response), state Medicaid variations, and proprietary commercial plan rules all shape how UM is executed.
It is also critical to understand that UM is intentionally focused on medical necessity qualification and separated from claims payment functionally. That being said, if authorization is required as a condition for payment and not received, then those services or treatments will not be paid for by the health plan's coverage and member benefits.
Therefore, failing to account for this operational matrix results in denial churn, unnecessary appeals, provider abrasion, and downstream care delays. It’s not just about what care is appropriate — it’s about whether that care is authorized under the terms of that patient’s policy, in that plan, at that moment. Later in the series you’ll see me mention a “270/271 Eligibility & Benefits” transaction, which is the real-time transaction that surfaces this patient-level benefit detail before care is rendered.
For those wanting to learn more about Payers, the products and structures, consider visiting AHIP or AMCP.
So Then What Is Utilization Management (UM), Really?
UM is a clinical and administrative umbrella for activities that assess the appropriateness, cost, and timing of healthcare services. While most commentary centers on prior authorization, but PA or ePA (electronic Prior Auth) are just one piece. UM spans medical and pharmacy benefits and coverage where complexity is most easily described using a Four-Dimensional UM Model.
To fully understand and improve UM, we need a 4-dimensional model that reflects its real-world structure and execution. This model captures when UM occurs (Temporal), what it targets (Functional), how it's operationalized (Operational), and the infrastructure that enables it (Technical).
This is not just an academic framework. It’s a practical tool for providers, developers, and the MedTech/Life Sciences industry to understand how the UM ecosystem comes together so as to navigate future hurdles in care and innovation.
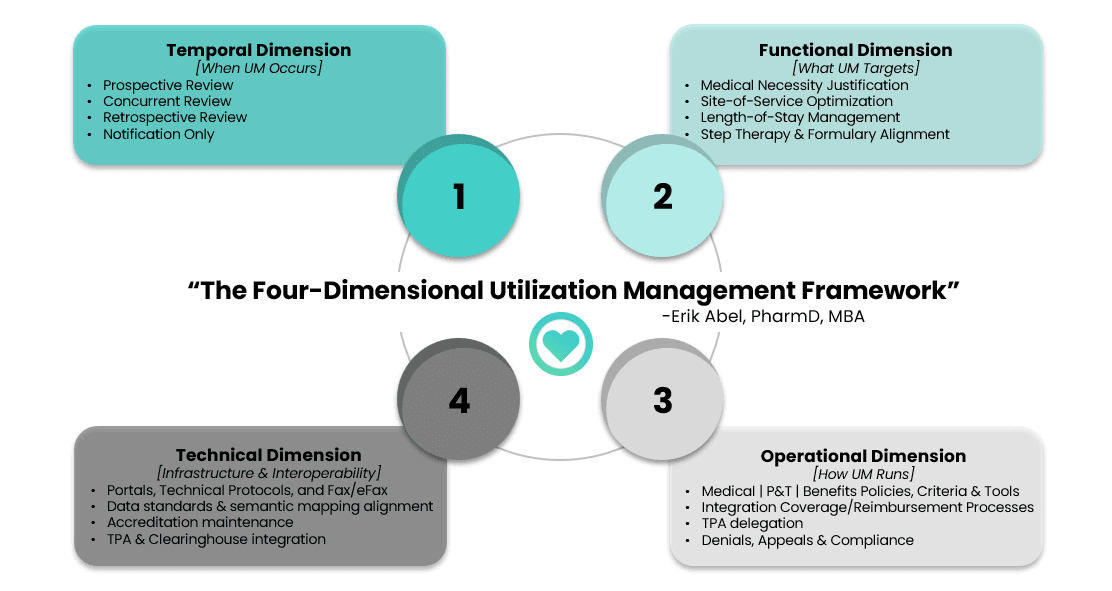
1 | Temporal Dimension of UM
This dimension governs when intervention happens along the care continuum, shaping access, cost, and clinical decision-making and also the level of friction and influence that is imposed on guidance as a contingency of coverage for across access, payment, and provider behavior differently. Note that misalignment between these can cause friction and waste.
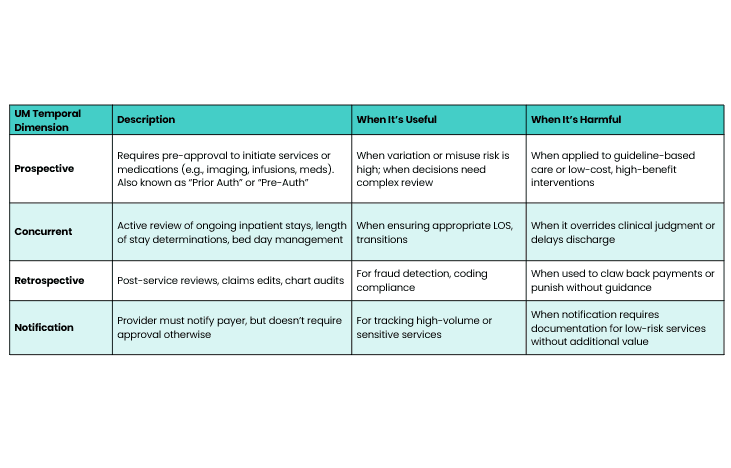
A "benefit silo" problem may still remain where different UM processes for the same intervention can be intentionally disparate depending on whether it's billed under the medical or pharmacy benefit as well as site of care. Thus quite the potential for a fragmented landscape with little coherence or predictability.
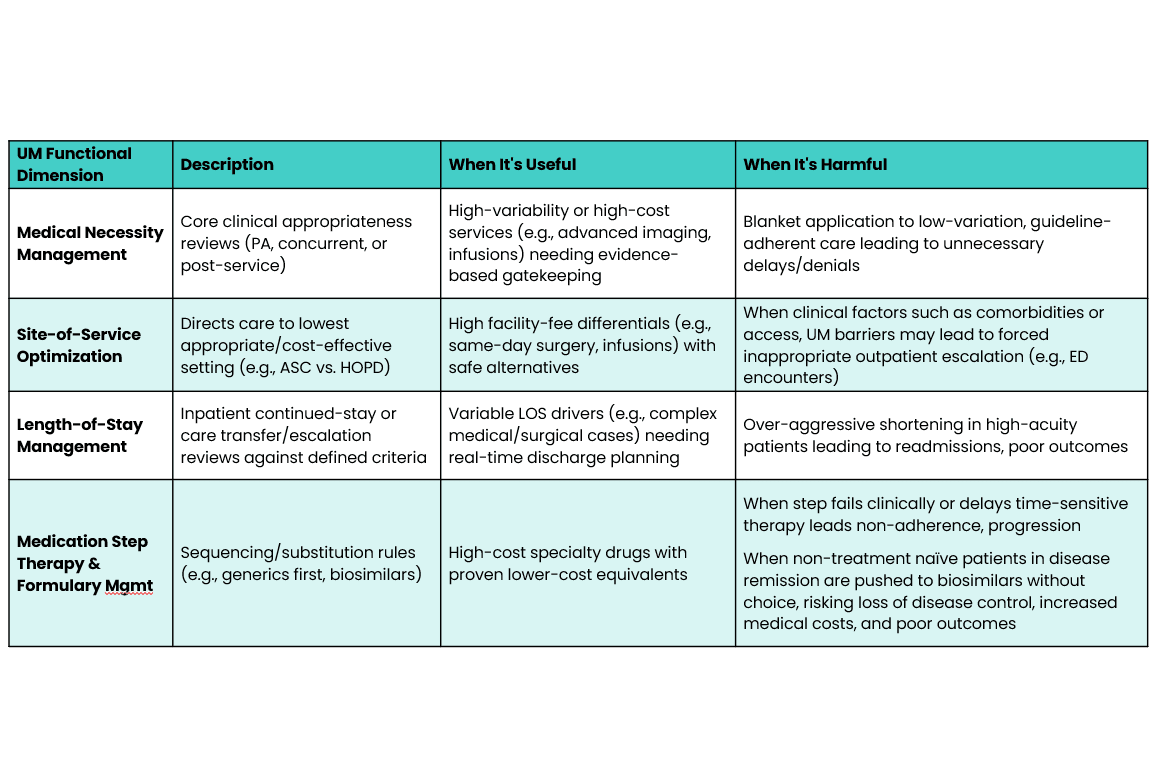
2 | Functional Dimension of UM
This defines the core intent of UM around the service or therapy in question, whether ensuring medical necessity, optimizing site-of-service, managing inpatient length-of-stay, or sequencing treatments through step therapy. It reflects the specific levers payers use to influence clinical and economic outcomes.
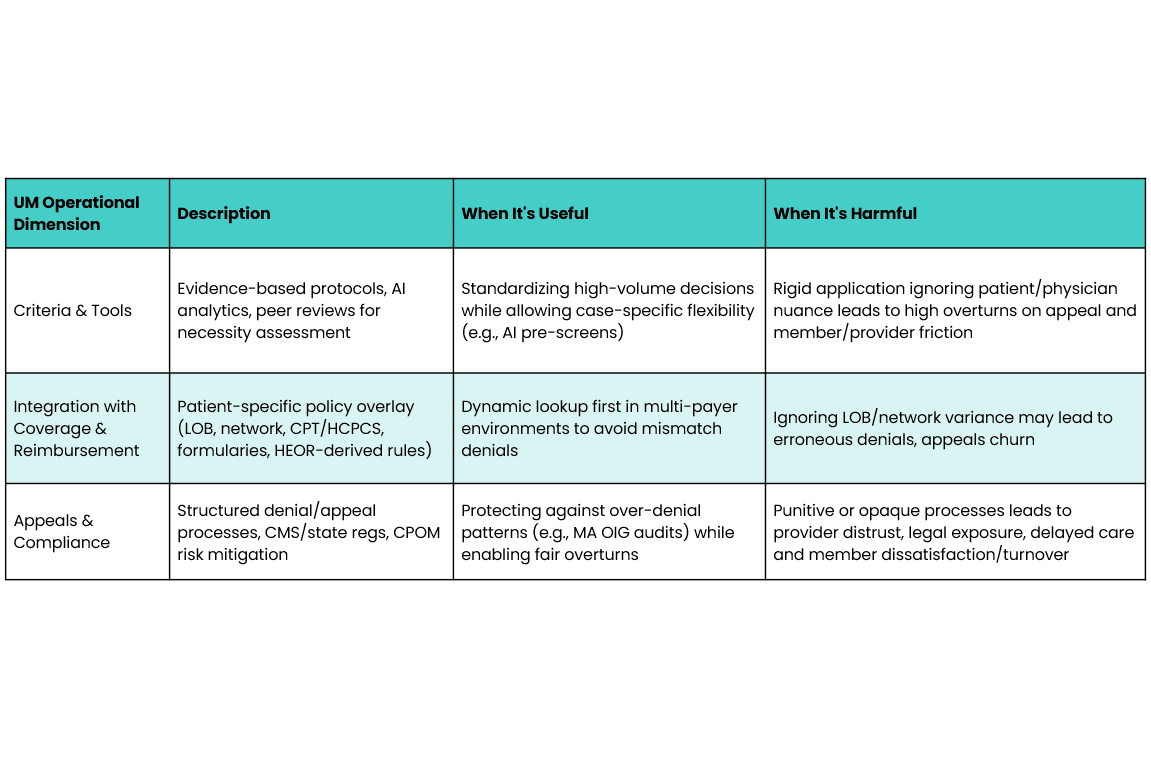
3 | Operational Dimension of UM
This dimension layers in the mechanics of implementation, from criteria application and appeals to benefit integration and policy overlays. It’s where payer rules, benefit design, and provider workflows intersect with high impact on compliance, denials, and member experience. I cannot overemphasize the communication demand required operationally with UM where health plans are held to regulatory standards that can vary across lines of business - some being state regulated while others are federally regulated with significate nuance. This remains a significant area of opportunity.
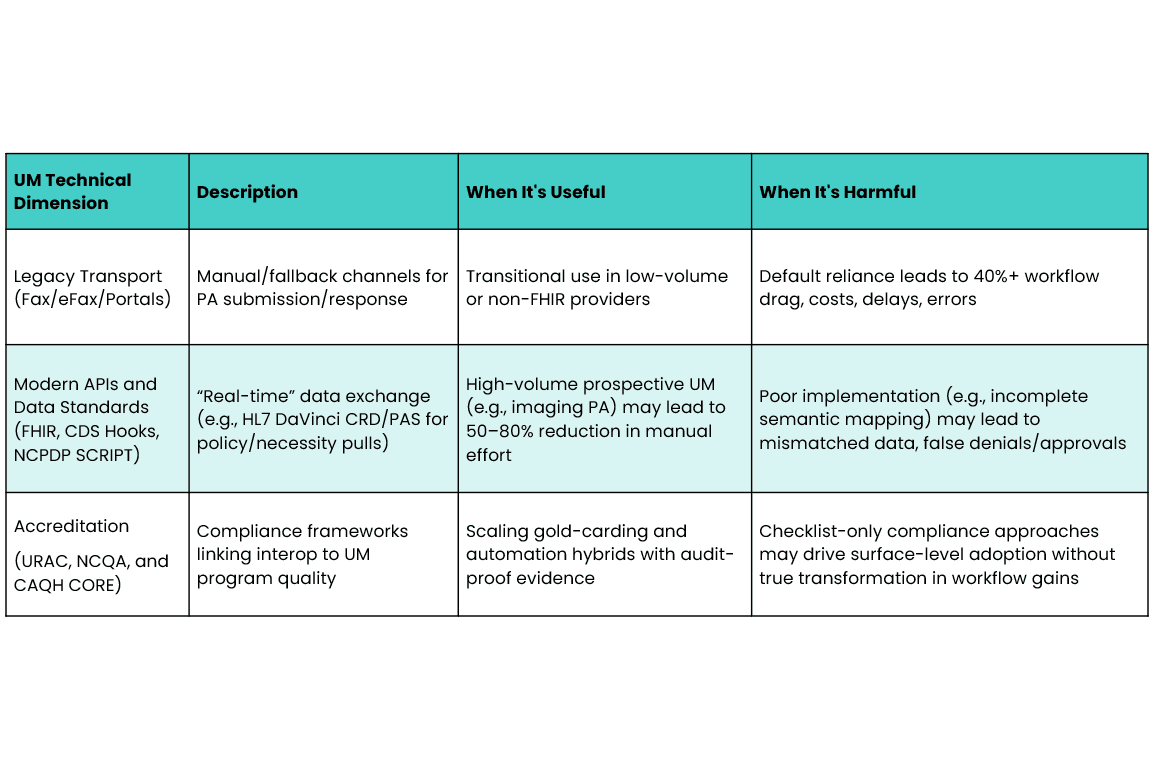
4 | Technical Dimension of UM
This last dimension has been the biggest focus of the industry with the aim of advancing the technical infrastructure and capabilities that enable (or hinder) UM activities including fax/e-fax, portals, platforms, APIs, HL7 Da Vinci Project FHIR approaches (e.g. CARIN Prior Auth and CARIN RTPBC)and data semantic interoperability enablers (e.g., RxNorm, LOINC, SNOMED, CPT, HCPCS, etc) to support complex data orchestration. This also becomes the space for EDI exchanges, clearinghouse interfaces, as well as integration of vendors and delegates third-party administrators (TPAs) who are involved in various aspects of medical or pharmacy benefits (e.g., PBMs).
Does UM Really Only Need a Technical "Tune-Up"?
To be clear, PA can work when used appropriately and despite pushes from many, it’s not going away anytime soon. Even the Centers for Medicare & Medicaid Services will be introducing PA in the near future where many will be left scratching their heads as this will expose the variability in Medicare Administrative Contractor (MAC) Local Coverage Determination (LCD) policies.
In Medicare Part D, PAs for certain drugs reduced utilization by 26.8% and lowered spending by $96 per beneficiary-year, with no reported adverse effect on outcomes. [1,4]
But instead of targeting high-variability, low-evidence use cases, PA is often applied where it's least needed like radiation oncology, which accounts for only 3–4% of cancer costs but is required in >50% of cases. [3]
This reflects a deeper issue: payment rules, coverage policies, and clinical workflows are built on outdated ontologies.
- Payers enforce coverage based on claims logic based on administrative data ontologies
- Clinicians use evidence-based guidelines and literature to guide decisions…none of which are defined for alignment to administrative data ontologies
- Providers operate in workflows “divorced” from reimbursement triggers
- Patients are left navigating opacity including delays, substitutions, or denials they can’t predict or influence
We've built "solutions" that optimize steps without questioning if the steps themselves should exist.
Evidence Doesn’t Move Fast Enough
Some of this misalignment is due to lagging evidence integration. Consider the following:
- It takes 9 years on average for clinical research to make it into guidelines [9]
- Payer policy integration of published evidence often lags at least 1-3 years behind published evidence
- Even after guideline updates, clinical practice adoption can take another 6–14 years, with a median of 14 years from guideline recommendation to 90% uptake [10,11]
- Meanwhile, about half of guidelines are "outdated" within 5.8 years [12]
So even when new therapies emerge or consensus evolves, coverage policy and clinical behavior often remain out of sync for over a decade. Utilization Management policy then activates blunt enforcement tools for outdated foundations.
A Final Rule With Real Teeth…But Blind Spots
In February 2024, Centers for Medicare & Medicaid Services finalized the Interoperability and Prior Authorization Final Rule (CMS-0057-F) that signals a significant step toward process standardization.[13] Entities impacted by CMS-0057 must meet HL7 FHIR-based API requirements by January 2027. In the meantime, CMS has since exercised enforcement discretion of the X12 278 transaction for HIPAA-covered entities that perform PA workflows electronically using HL7 FHIR. It is anticipated that use of the WEDI X12 278 will decrease as industry approaches regulatory deadlines. The Final Rule includes:
- Required FHIR-based APIs for identifying PA requirements and documentation [13]
- Response deadlines: 72 hours for urgent, 7 days for nonurgent requests [13]
- Payers must provide clear denial reasons and publish PA metrics annually [13]
- Estimated savings: $1.15B in 2027, $2.10B by 2036 [13,14].
But there’s a major gap: the rule excludes pharmacy benefits (Parts B and D), due to differing NCPDP data standards for PA - although payers can still share this information by API. Of note, pharmacy is estimated to account for 35% of PAs and 57% of projected savings [15].
The digital plumbing will help….but it still won’t solve the upstream logic problem.
What Might Actually Fix This
Large Language Models (LLMs) and AI-based tools including OpenEvidence, OpenAi's ChatGPT, Anthropic's Claude, Atropos Health, Abridge, Hippocratic AI and many others have proven to be valuable for many use cases, but have not seemed to be pointed at one key UM problem they are most well suited to solve. As we have partially peeled back the layers of complexity, rather than using these tools to automate coverage appeals after denials occur, it would seem the bigger value would be to compress the evidence-to-coverage-to-practice lag before misalignment creates friction:
- Informing and supporting more timely payer policy updates and provider-facing decision support
- Synthesizing clinical trials and real-world evidence in more pragmatic “real-time”
- Mapping new evidence or guidelines to billing codes, NDCs, and coverage frameworks for actuarial analysis and forecasting review
If used correctly, these tools could help achieve what UM originally set out to do: optimize care, reduce waste, and build trust between payer and provider on what value-oriented, evidence backed care truly can be.
What Comes Next
If UM and prior authorization are symptoms and NOT the root cause, then real transformation lies in how we structure and align value for the system beneath it.
Follow-on for more “unpacking”:
- In Part 2: Behind the Curtain, I’ll explain the UM TPA vendor ecosystem and who actually pulls the operational levers
- In Part 3: The Digital Highway, I’ll look at why standards like HL7 FHIR, X12 278, NCPDP, and CARIN remain as amazing steps forward, but also cover some limitations in utility as well as what that means for interoperability
- Lastly, in Part 4: Reimagining UM, we’ll explore performance-based pathways like gold carding, where providers with high-approval rates gain exemption from prior auth altogether. The early data is promising, but these models depend on smarter logic, not just looser guardrails.
Final Thoughts for Today
UM reform isn't about bypassing controls. It’s about building smarter systems that learn, trust, and adapt. UM was built to ensure the right care at the right time. Too often, it now achieves the opposite.
It’s time to redesign from first principles, not just digitize dysfunction.
References:
1. Howell S, Yin PT, Robinson JC. Quantifying the economic burden of drug utilization management on payers, manufacturers, physicians, and patients. Health Aff (Millwood). 2021; 40(8):1206-1214. doi: 10.1377/hlthaff.2021.00036
2. Murphy J, Beauchamp N, Sun KJ, et al. Adverse effects of health plan prior authorization on clinical effectiveness and patient outcomes: a systematic review. Am J Med. 2025;138(2):132–43. doi:10.1016/j.amjmed.2024.07.010
3. Chen WC, Carpenter C, Sidiqi B, et al. Integrating prior authorization into clinical workflows for care access and practitioner experience. JAMA Netw Open. 2025;8(1):e250011. doi:10.1001/jamanetworkopen.2025.0011
4. Gotlieb E, Joseph B, Blank L, Jetté N. Barriers and consequences of prior authorization for neurologic medications. JAMA Neurol. 2025;82(4):427–35. doi:10.1001/jamaneurol.2024.5912
5. American Medical Association. One in three doctors has seen prior auth lead to serious adverse event [Internet]. Chicago (IL): AMA; 2023 Mar [cited 2026 01 14]. Available from: https://www.ama-assn.org/delivering-care/patient-support-advocacy/1-3-doctors-has-seen-prior-auth-lead-serious-adverse
6. CAQH. 2024 CAQH Index Report: Measuring progress in adoption of electronic business transactions [Internet]. Washington (DC): Council for Affordable Quality Healthcare; 2024 Jan [cited 2024 Dec 29]. Available from: https://www.caqh.org/sites/default/files/2024-01/2024-caqh-index.pdf
7. 2024 AMA prior authorization physician survey. AMA. Accessed February 24, 2025. https://www.ama-assn.org/system/files/prior-authorization-survey.pdf
8. Chino F, Baez A, Elkins IB, et al. The patient experience of prior authorization for cancer care. JAMA Netw Open. 2023;6(10):e2315526. doi: 10.1001/jamanetworkopen.2023.38182
9. Borchert F, Wullenweber P, Oeser A, et al. High-precision information retrieval for rapid clinical guideline updates. NPJ Digit Med. 2025;8(1):14. doi:10.1038/s41746-024-01078-2
10. Khan S, Chambers D, Neta G. Revisiting time to translation: implementation of evidence-based practices in cancer control. Cancer Causes Control. 2021;32(5):479–86. doi:10.1007/s10552-021-01401-1
11. Putera M, Roark R, Lopes RD, Udayakumar K, Peterson ED, Califf RM, Shah BR. Translation of acute coronary syndrome therapies: from evidence to routine clinical practice. Am Heart J. 2015 Feb;169(2):266-73. doi: 10.1016/j.ahj.2014.09.015. Epub 2014 Nov 12.
12. Shekelle PG, Ortiz E, Rhodes S, et al. Validity of the Agency for Healthcare Research and Quality clinical practice guidelines: how quickly do guidelines become outdated? JAMA. 2001;286(12):1461–7. doi:10.1001/jama.286.12.1461
13. Centers for Medicare & Medicaid Services. CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) [Internet]. Baltimore (MD): CMS; 2024 Jan [cited 2024 Dec 29]. Available from: https://www.cms.gov/files/document/cms-0057-f.pdf
14. Kannarkat JT, Warring W, Brennan T. Advancing Interoperability and Prior Authorization Reform. JAMA Health Forum. 2024;5(6):e241193. doi:10.1001/jamahealthforum.2024.1193